

When Did The Us Start Rationing Health Care Services
Healthcare rationing in the United states of america exists in various forms. Access to private health insurance is rationed on price and ability to pay. Those unable to afford a health insurance policy are unable to larn a individual plan except by employer-provided and other chore-attached coverage, and insurance companies sometimes pre-screen applicants for pre-existing medical conditions. Applicants with such conditions may be declined cover or pay higher premiums and/or accept extra conditions imposed such as a waiting flow.[1] [2]
The poor are given access to Medicaid, which is restricted by income and asset limits by means-testing, and other federal and land eligibility regulations employ. Health maintenance organizations (HMOs), which are mutual among the residue of the population, restrict access to treatment by financial and clinical access limits.[3] [ folio needed ] Those 65 and older and a few others besides qualify for Medicare, only it also has many restrictions.
In the media and in academia, some accept advocated explicit healthcare rationing to limit the cost of Medicare and Medicaid. They argue that a proper rationing mechanism would be more equitable and cost-effective.[4] [5] [half-dozen]
The Congressional Budget Office (CBO) has argued that health intendance costs are the master driver of regime spending in the long term.[7]
Background [edit]
Peter Singer wrote for the New York Times Mag in July 2009 that healthcare is rationed in the United States:[4]
"Health intendance is a scarce resource, and all scarce resource are rationed in one way or another. In the United States, almost health care is privately financed, and and then most rationing is by price: yous get what you lot, or your employer, can afford to insure y'all for. Merely our electric current system of employer-financed health insurance exists only because the federal government encouraged information technology past making the premiums tax deductible. That is, in effect, a more than than $200 billion regime subsidy for health care. In the public sector, primarily Medicare, Medicaid and hospital emergency rooms, wellness care is rationed past long waits, high patient copayment requirements, low payments to doctors that discourage some from serving public patients and limits on payments to hospitals."
David Leonhardt wrote in the New York Times in June 2009 that rationing soon an economic reality: "The choice isn't between rationing and non rationing. It's betwixt rationing well and rationing badly. Given that the United states of america devotes far more of its economy to health care than other rich countries, and gets worse results by many measures, information technology's hard to fence that nosotros are at present rationing very rationally." He wrote that there are 3 primary means the United states of america rations healthcare:[vi]
- The increases in healthcare premiums reduce worker pay. In other words, more expensive insurance premiums reduce the growth in household income, which forces tradeoffs between healthcare services and other consumption.
- The increases also forestall smaller companies from affording health insurance for their workers.
- The cost prevents the certain types of intendance from being provided.
During 2007, virtually 45% of Usa healthcare expenses were paid for by the government.[8] In 2009, an estimated 46 meg individuals in the U.s.a. did not accept health insurance coverage. In 2008, Tia Powell led a New York Country work group to set up guidelines for rationing ventilators during a potential flu pandemic.[9]
Methods used [edit]
By insurance companies [edit]
Dr. Gerald Grumet has chronicled how private insurers and third party payers filibuster and impede the utilization of medical services through creating inconvenience and confusion for both patients and physicians through circuitous claims review processes with layers of authoritative handling that replace the autonomy of treating physicians.[10]
President Obama noted that US healthcare was rationed based on income, blazon of employment, and pre-existing medical conditions, with most 46 one thousand thousand uninsured. He stated that millions of Americans were denied coverage or face higher premiums considering of pre-existing medical atmospheric condition.[1]
In an e-mail to Obama supporters, David Axelrod wrote, "Reform volition terminate 'rationing' - not increase information technology.... Information technology's a myth that reform volition mean a 'government takeover' of wellness care or atomic number 82 to 'rationing.' To the contrary, reform will forbid many forms of rationing that are currently existence used by insurance companies."[11]
A 2008 report by researchers at the Urban Institute found that health spending for uninsured non-elderly Americans was just about 43% of health spending for similar, privately-insured Americans. That unsaid rationing past price and ability to pay.[12]
Fareed Zakaria wrote that only 38% of minor businesses provided wellness insurance for their employees during 2009, versus 61% in 1993, because of rising costs.[13]
An investigation by the House Subcommittee on Oversight and Investigations showed that wellness insurers WellPoint Inc., UnitedHealth Group and Assurant Inc. canceled the coverage of more than xx,000 people, allowing the companies to avoid paying more than than $300 million in medical claims over five years. It also found that policyholders with breast cancer, lymphoma, and more than m other weather condition were targeted for rescission and that employees were praised in performance reviews for terminating the policies of customers with expensive illnesses.[xiv]
Private and public insurers all have their own drug formularies through which they prepare coverage limitations, which may include referrals to the insurance company for a decision on whether the visitor will approve its share of the costs. American formularies make generalized coverage decisions by class, with cheaper drugs at ane end of the calibration and more than expensive drugs with more conditions for referral and possible denial at the other end. Not all drugs may exist in the formulary of every company, and consumers are advised to cheque the formulary before they buy insurance.[15]
The phenomena known equally medical bankruptcy is unheard of in countries with universal health care in which medical copayments are low or no nonexistent.[ citation needed ] In the United States, nonetheless, enquiry shows[ who? ] that many bankruptcies take a strong medical component, fifty-fifty among the insured.[ commendation needed ] Medical insurance before the Affordable Care Act allowed annual caps or lifetime caps on coverage, and the loftier cost of care made information technology common for insured persons to endure bankruptcy after breaching those limits.[ citation needed ]
By price [edit]
A July 2009 NPR article quoted various doctors describing how America rations healthcare. Dr. Arthur Kellermann said: "In America, we strictly ration health intendance. We've done information technology for years.... Merely in dissimilarity to other wealthy countries, nosotros don't ration medical care on the ground of need or anticipated benefit. In this land, nosotros mainly ration on the ability to pay. And that is especially evident when yous examine the plight of the uninsured in the United States."[16]
Rationing by price ways accepting that there is no triage co-ordinate to need. Thus, in the individual sector, it is accepted that some people become expensive surgeries such as liver transplants or not-life-threatening ones such every bit corrective surgery, when others fail to become cheaper and much more cost-effective intendance such as prenatal care, which could save the lives of many fetuses and newborn children. Some places, similar Oregon for case, explicitly ration Medicaid resources past using medical priorities.[17]
Polling has discovered that Americans are much more probable than Europeans or Canadians to forgo necessary health intendance (such not seeking a prescribed medicine) on the grounds of cost.[ commendation needed ]
Co-ordinate to a recent survey deputed past Wolters Kluwer, the majority of physicians and nurses (79%) say the price to the patient influences the treatment choices or recommendations the provider makes.[xviii]
Rationing past pharmaceutical companies [edit]
Pharmaceutical manufacturers oftentimes charge much more for drugs in the United States than they charge for the same drugs in Great britain, where they know that a higher price would put the drug outside the cost-effectiveness limits applied by regulators such every bit NICE. American patients, even if they are covered by Medicare or Medicaid, oftentimes cannot afford the copayments for drugs, which is rationing based on ability to pay.[four]
Rationing past government control [edit]
After the death of Coby Howard in 1987[19] Oregon began a programme of public consultation to decide which procedures its Medicaid program should comprehend in an attempt to develop a transparent process for prioritizing medical services. Howard died of leukaemia, which was not funded. His mother spent the last weeks of his life trying to heighten $100,000 to pay for a bone marrow transplant, but the boy died before treatment could begin. John Kitzhaber began a campaign arguing that thousands of low-income Oregonians lacked access to even basic wellness services, much less access to transplants. A panel of experts was appointed, the Health Services Commission, to develop a prioritized listing of treatments. The state legislators decided where on the list of prioritised procedures the line of eligibility should exist drawn. In 1995 in that location were 745 procedures, 581 of which were eligible for funding.[20]
Republican Newt Gingrich argued that the reform plans supported by President Obama expand the command of government over healthcare decisions, which he referred to as a type of healthcare rationing. He expressed business organisation that although in that location is cypher in the proposed laws that would constitute rationing, the combination of three factors would increase pressure on the government to ration intendance explicitly for the elderly:[21] an expanded federal bureaucracy, the pending insolvency of Medicare within a decade, and the fact that 25% of Medicare costs are incurred in the final twelvemonth of life.
Princeton Professor Uwe Reinhardt wrote that both public and private healthcare programs can ration and rebutted the concept that governments lone impose rationing: "Many critics of the current health reform efforts would have us believe that but governments ration things.... On the other paw, these same people believe that when, for similar reasons, a private wellness insurer refuses to pay for a particular procedure or has a price-tiered formulary for drugs – eastward.g., asking the insured to pay a 35 percent coinsurance rate on highly expensive biologic specialty drugs that effectively put that drug out of the patient'south reach — the insurer is not rationing wellness care. Instead, the insurer is merely assuasive "consumers" (formerly "patients") to use their discretion on how to utilise their own money. The insurers are said to be managing prudently and efficiently, forcing patients to trade off the benefits of health care against their other budget priorities."[22]
During 2009, former Alaska Governor Sarah Palin wrote confronting rationing by government entities, referring to what she interpreted as such an entity in current reform legislation equally a "death panel" and "downright evil." Defenders of the programme indicated that the proposed legislation, H.R. 3200, would let Medicare for the first time to cover patient-md consultations almost end-of-life planning, including discussions about drawing up a living will or planning hospice treatment. Patients would be immune but not required to seek out such advice on their own. The provision would limit Medicare coverage to i consultation every five years.[23] However, as governor, Palin had supported such end of life counseling and accelerate directives from patients in Alaska in 2008.[24]
Ezra Klein described in the Washington Postal service how polls indicate senior citizens are increasingly resistant to healthcare reform because of concerns about cuts to the existing Medicare programme that may be required to fund it. That is creating an unusual and potent political alliance, with Republicans arguing to protect the existing Medicare program although they historically opposed that and other major entitlement programs.[25] The CBO scoring of the proposed H.R. 3200 (America's Affordable Health Choices Act of 2009) included $219 billion in savings over 10 years, some of which would come up from Medicare changes.[26]
By economic value added [edit]
A concept called "quality-adjusted life year" (QALY - pronounced "qualy") is used by Australian Medicare to measure the cost-do good of applying a particular medical process. Information technology reflects the quality and the quantity of life added past incurring a particular medical expense. The measure has been used for over 30 years in the country's universal single-payer healthcare system and has been implemented in several other countries to help with rationing decisions. Australia applies QALY measures to control costs and ration care and allows private supplemental insurance for those who can beget information technology.[4]
By comparative effectiveness research [edit]
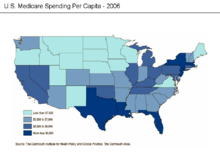
Medicare spending per person varied significantly beyond states in 2006
Several handling alternatives may be available for a given medical status, with significantly different costs but no statistical departure in consequence. Such scenarios offer the opportunity to maintain or improve the quality of care while significantly reducing costs through comparative effectiveness research. Writing in the New York Times, David Leonhardt described how the cost of treating the most common class of early-phase, slow-growing prostate cancer ranges from an average of $two,400 (watchful waiting to come across if the condition deteriorates) to as high equally $100,000 (radiations beam therapy):[27]
Some doctors swear by i treatment, others by some other. But no 1 actually knows which is best. Rigorous research has been scant. To a higher place all, no serious study has establish that the loftier-technology treatments do better at keeping men salubrious and alive. Near die of something else before prostate cancer becomes a problem.
Co-ordinate to economist Peter A. Diamond and research cited by the Congressional Upkeep Office (CBO), the cost of healthcare per person in the US also varies significantly by geography and medical center, with little or no statistical difference in outcome:[28]
Although the Mayo Clinic scores to a higher place the other two [in terms of quality of outcome], its cost per beneficiary for Medicare clients in the last six months of life ($26,330) is nearly half that at the UCLA Medical Center ($l,522) and significantly lower than the cost at Massachusetts General Hospital ($xl,181)...The American taxpayer is financing these large differences in costs, just we have little evidence of what benefit we receive in exchange.
Comparative effectiveness inquiry has shown that meaning cost reductions are possible. Office of Direction and Upkeep (OMB) Director Peter Orszag stated: "Nearly thirty percentage of Medicare's costs could be saved without negatively affecting health outcomes if spending in loftier- and medium-cost areas could exist reduced to the level of depression-cost areas."[29]
President Obama has provided more $1 billion in the 2009 stimulus package to jumpstart Comparative Effectiveness Research (CER) and to finance a federal CER advisory council to implement that idea. Economist Martin Feldstein wrote in the Wall Street Journal, "Comparative effectiveness could become the vehicle for deciding whether each method of treatment provides plenty of an improvement in health intendance to justify its cost."[30]
By authorities [edit]
Former Republican Secretary of Commerce Peter George Peterson indicated that some course of rationing is inevitable and desirable considering the country of US finances and the trillions of dollars of unfunded Medicare liabilities. He estimated that 25 to 33% of healthcare services are provided to those in the concluding months or year of life and advocated restrictions if quality of life cannot be improved. He likewise recommended for a budget to exist established for government healthcare expenses past establishing spending caps and pay-as-you-get rules that crave tax increases for any incremental spending. He has indicated that a combination of tax increases and spending cuts volition be required. He advocated addressing those issues under the custodianship of a fiscal reform commission.[5]
Arizona modified its Medicaid coverage rules because of a budget trouble that included denying care for expensive treatments such as organ transplants to Medicaid recipients, including those who had previously been promised funding.[31] MSNBC'southward Keith Olbermann and others[ co-ordinate to whom? ] have dubbed Governor Jan Brewer and the state legislatures as a real life death console[ citation needed ] because many of those poor people who are now beingness denied funding will lose their lives or have health considering of the political decision.
By historic period [edit]
In the Us, the discussion on rationing healthcare for the elderly began to exist noticed widely in 1983 when economist Alan Greenspan asked "whether information technology is worth information technology" in referring to the use of thirty% of the Medicare upkeep on 5–6% of those eligible who then die within a year of receiving treatment. In 1984, the Democratic governor of Colorado, Richard Lamm, was widely quoted only claimed to have been misquoted as maxim that the elderly "have a duty to die and get out of the way."[32]
Medical ethicist Daniel Callahan's 1987 Setting Limits: Medical Goals in an Crumbling Society [33] discusses whether healthcare should exist rationed by historic period. He calls the elderly "a new social threat" and selfish and for historic period to exist used every bit a benchmark in limiting healthcare. Callahan's book has been widely discussed in the America media, including the New York Times, the Washington Post, the Wall Street Periodical, and "but about every relevant professional and scholarly journal and newsletter."[34] 1 of the major arguments against such age-based rationing is the fact that chronological age, by itself, is a poor indicator of health.[35] Another major argument against Callahan'southward proposal is that it inverts the Western tradition by making decease a possible good and life a possible evil. Amherst Higher Jurisprudence Professor Robert Laurence Barry called Callahan's view "medical totalitarianism."[36] [ folio needed ] One book-length rebuttal to Callahan from half-a-dozen professors who held a conference at the University of Illinois College of Constabulary in October 1989 was in 1991'south Set No Limits: a Rebuttal to Daniel Callahan's Proposal to Limit Wellness, edited past Robert Laurence Barry and Gerard V. Bradley, a visiting professor of religious studies at the University of Illinois at Urbana–Champaign.[36] [ page needed ]
Arguments in favor [edit]
Australian philosopher Peter Vocalist argued for rationing processes:[ane]
"Rationing health care means getting value for the billions we are spending by setting limits on which treatments should be paid for from the public purse. If we ration we won't be writing blank checks to pharmaceutical companies for their patented drugs, nor paying for any procedures doctors choose to recommend. When public funds subsidize health care or provide information technology directly, information technology is crazy not to try to get value for money. The fence over health care reform in the United States should kickoff from the premise that some form of health care rationing is both inescapable and desirable. Then nosotros can ask, What is the best way to practice it?"
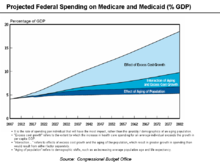
Medicare and Medicaid Spending equally a percentage of GDP
The Congressional Budget Role reported in June 2008:[seven]
"Future growth in spending per casher for Medicare and Medicaid—the federal regime's major health intendance programs—will be the near important determinant of long-term trends in federal spending. Changing those programs in ways that reduce the growth of costs—which will be difficult, in part because of the complication of health policy choices—is ultimately the nation'due south central long-term challenge in setting federal fiscal policy... total federal Medicare and Medicaid outlays will rising from 4 percent of Gdp in 2007 to 12 percent in 2050 and 19 percent in 2082—which, as a share of the economic system, is roughly equivalent to the total amount that the federal authorities spends today. The bulk of that projected increase in health intendance spending reflects higher costs per casher rather than an increase in the number of beneficiaries associated with an aging population."
In other words, all other federal spending categories (such as Social Security, defense force, education, and transportation) would crave borrowing to be funded, which is not feasible.
President Obama stated in May 2009, "But nosotros know that our families, our economy, and our nation itself will non succeed in the 21st century if nosotros continue to be held down past the weight of speedily rise wellness care costs and a cleaved health care arrangement.... Our businesses will not be able to compete; our families volition not exist able to save or spend; our budgets will remain unsustainable unless we become health care costs under command."[37]
Healthcare rationing remained a political topic into 2017, with Bernie Sanders and Ted Cruz debating on CNN whether a unmarried-payer organisation would lead to healthcare rationing.[38]
See also [edit]
- Healthcare reform in the U.s.a.
- Healthcare reform debate in the United states of america
- Public opinion on wellness care reform in the United States
- Wellness care in the Us
- Death panel
References [edit]
- ^ a b c Obama, Barack (2009-08-fifteen). "Why Nosotros Need Healthcare Reform". The New York Times . Retrieved 2017-12-17 .
- ^ "Jim Jaffe, "Underground's Out—We Already Ration Medical Care", AARP Bulletin Today, July 30, 2009". Archived from the original on 2009-09-26. Retrieved 2009-09-29 .
- ^ Martin A. Strosberg; Joshua One thousand. Wiener; Brookings Institution; Robert Baker (1992). Rationing America'south medical care. ISBN978-0-8157-8197-4.
- ^ a b c d Vocaliser, Peter (2009-07-15). "Why We Must Ration Health Care". New York Times Magazine . Retrieved 2017-12-17 .
- ^ a b Peter M. Peterson on Charlie Rose-July iii 2009-Virtually 17 min in Archived 2012-03-19 at the Wayback Car
- ^ a b NYT-Leonhardt-Healthcare Rationing Rhetoric Overlooks Reality-June 2009
- ^ a b CBO Testimony
- ^ "Centers for Medicare and Medicaid Services-Pie Charts-2007" (PDF). Archived from the original (PDF) on 2009-09-02. Retrieved 2009-08-17 .
- ^ Cornelia Dean, Guidelines for Epidemics: Who Gets a Ventilator?, The New York Times, March 25, 2008
- ^ "Health Care Rationing Through Inconvenience: The Third Party's Hole-and-corner Weapon," Grumet, Gerald W., M.D., New England Journal of Medicine. 1989 Aug 31; 321(9): 607-611.
- ^ Huffington Mail service-Nutter-Axelrod's Whitehouse E-mail-Baronial 2009
- ^ NYT-Reinhardt-Rationing Healthcare-What Does information technology Hateful?
- ^ Washington Postal service-Zakaria-More than Crises Needed?-August 2009
- ^ How Would Yous Ration Health Care? Bloomberg Businessweek, citing LA Times commodity
- ^ http://www.ahip.org/content/default.aspx?bc=41%7C329%7C20888
- ^ NPR-Healthcare Rationing Already Exists-July 2009
- ^ Time Magazine-Ethics: Rationing Medical Intendance-Sept 09
- ^ Mending Healthcare in America 2020: Consumers + Cost
- ^ "A Transplant for Coby: Oregon Boy'southward Death Stirs Argue Over State Decision Not to Pay for High-Risk Treatments". Los Angeles Times. 28 December 1987. Retrieved nineteen May 2015.
- ^ Perry, Philip; Hotze, Timothy (Apr 2011). "Oregon's Experiment with Prioritizing Public Health Care Services". AMA Periodical of Ethics. thirteen (4): 241–247. doi:10.1001/virtualmentor.2011.thirteen.4.pfor1-1104. PMID 23131332. Retrieved 19 May 2015.
- ^ "Newt Gingrich, Los Angeles Times, Atlanta Periodical-Constitution, Baronial xvi, 2009 "Healthcare Rationing-Existent Scary"". Archived from the original on 2009-08-22. Retrieved 2009-09-29 .
- ^ NYT-Rheinhardt-Rationing Healthcare: What Does It Mean?-July 2009
- ^ Farber, Dan (2009-08-08). "Palin Weighs In On Healthcare Reform". cbsnews.com . Retrieved 2017-12-17 .
- ^ Office of the Governor of Alaska-Healthcare Decisions Day
- ^ Washington Post-Ezra Klein-No Regime Healthcare! (Except for Mine)-August 2009
- ^ CBO Written report-July 14
- ^ NYT-Leonhardt-In Health Reform, A Cancer Offers and Acid Exam
- ^ Peter Diamond-Healthcare and Behavioral Economics-May 2008
- ^ The New Yorker-Gawande-The Cost Puzzler-June 2009
- ^ WSJ-Feldstein-Obamacare All About Rationing-August 2009
- ^ Lacey, Marc (December 2, 2010). "Arizona Cuts Financing for Transplant Patients". The New York Times.
- ^ "Gov. Lamm asserts elderly, if very sick, have 'DUTY TO DIE'". New York Times. March 29, 1984.
- ^ Setting Limits: Medical Goals in an Aging Gild. Daniel Callahan. Edition reprint. Georgetown University Press, 1995 (orig. pub. 1987). ISBN 0-87840-572-0.
- ^ Growing onetime in America. Beth B. Hess, Elizabeth Warren Markson. 4th Ed. Transaction Publishers, 1991. ISBN 0-88738-846-9. p. 329.
- ^ Aging: Concepts and Controversies. Harry R. Moody, Director of Academic Affairs, AARP. 5th Ed. Pino Forge Printing, 2006. ISBN one-4129-1520-1. p.301.
- ^ a b Barry, Robert 50; Bradley, Gerard (1991). Set No Limits: a Rebuttal to Daniel Callahan'south Proposal to Limit Health Care. Academy of Illinois Press. ISBN0-252-01860-5.
- ^ Obama, Barack (2009-05-16). "Two Pillars of a New Foundation". RealClearPolitics.com . Retrieved 2017-12-17 .
- ^ King, Robert (Feb 7, 2017). "Cruz, Sanders trade jabs over healthcare rationing". Washington Examiner. United states. Retrieved February 27, 2018.
External links [edit]
- Reforming American Healthcare from The Economist
- White Business firm Council of Economic Advisors - The Economic Case for Healthcare Reform-Report-June 2009

Source: https://en.wikipedia.org/wiki/Healthcare_rationing_in_the_United_States
Posted by: murrayhisclowed.blogspot.com
0 Response to "When Did The Us Start Rationing Health Care Services"
Post a Comment